6 mg/2 ml
For the use of a Registered Medical Practitioner or a Hospital or a Institution only.
%20Structure.jpg)
Administration :
For rapid bolus intravenous use only.
SOLADENO should be given as a rapid bolus by the peripheral intravenous route. To be certain the solution reaches the systemic circulation, it should be administered either directly into a vein or, if given into an IV line, it should be given as close to the patient as possible and followed by a rapid saline flush.
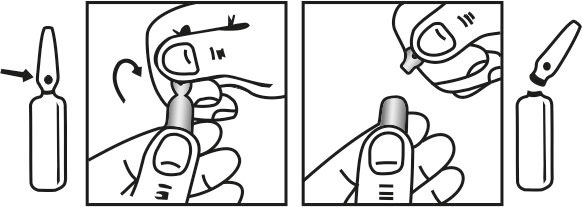
INSTRUCTION FOR USE OF AMPOULE :
The ampoule used in this product is equipped with O.P.C (One Point Cut) opening system. No ampoule file is needed to open the ampoule. The neck of the ampoule is prescored at the point of constriction. A coloured dot on the ampoule head helps to orientate the ampoule. Take the ampoule and face the coloured dot. Let the solution at the head of the ampoule to flow down by shaking or a gentle stroke. The ampoule opens easily by placing the thumb on the coloured dot and gently pressing downwards as shown.
Dosage :
Adenosine is intended for hospital use only with monitoring and cardiorespiratory resuscitation equipment available for immediate use. It should be administered by rapid IV bolus injection according to the ascending dosage schedule below. To be certain the solution reaches the systemic circulation administer either directly into a vein or into an IV line. If given into an IV line it should be injected as proximally as possible, and followed by a rapid saline flush.Adenosine should only be used when facilities exist for cardiac monitoring. Patients who develop high-level AV block at a particular dose should not be given further dosage increments.
Therapeutic dose :
Adult :
Initial dose : 3 mg given as a rapid intravenous bolus (over 2 seconds).
Second dose : If the first dose does not result in elimination of the supraventricular tachycardia within 1 to 2 minutes, 6 mg should be given also as a rapid intravenous bolus.
Third dose : If the second dose does not result in elimination of the supraventricular tachycardia within 1 to 2 minutes. 12 mg should be given also as a rapid intravenous bolus. Additional or higher doses are not recommended.
Children : No controlled paediatric study has been undertaken. Published uncontrolled studies show similar effects of adenosine in adults and children : effective doses for children were between 0.0375 and 0.25 mg/kg.
Elderly : See dosage recommendations for adults.
Diagnostic dose : The above ascending dosage schedule should be employed until sufficient diagnostic information has been obtained.
Pregnancy : Teratogenic Effects : Pregnancy Category C