500 mcg/ 2 ml
For the use of a Registered Medical Practitioner or a Hospital or a Institution only.
DIXISOL (Digoxin) is a cardiotonic glycoside obtained from the leaves of Digitalis lanata Ehrhart (Family- Scrophulariaceae). Chemically, digoxin is 3b-[(2,6-Dideoxy-b-D-ribo-hexopyranosyl-(1®4)-2,6-dideoxy-b-D-ribo-hexopyranosyl-(1®4)-2,6-dideoxy-b-D-ribo-hexopyranosyl)oxy]-12b,14-dihydroxy-5b-card-20(22)-enolide. The molecular formula is C41H64O14 and molecular weight is 781.
STRUCTURAL FORMULA :
Its structural formula is :
-Structure.jpg)
DIXISOL is a sterile, nonpyrogenic, clear, colorless solution filled in amber ampoule of suitable size.
COMPOSITION :
Each ml contains :
ACTIONS :
Digoxin increases contractility of the myocardium by direct activity. This effect is proportional to dose in the lower range and some effect is achieved with quite low dosing; it occurs even in normal myocardium although it is then entirely without physiological benefit. The primary action of digoxin is specifically to inhibit adenosine triphosphatase and thus sodium-potassium (Na+-K+) exchange activity, the altered ionic distribution across the membrane resulting in an augmented calcium ion influx and thus an increase in the availability of calcium at the time of excitation-contraction coupling. The potency of digoxin may therefore appear considerably enhanced when the extracellular potassium concentration is low, with hyperkalaemia having the opposite effect. Digoxin exerts the same fundamental effect of inhibition of the Na+-K+ exchange mechanism on cells of the autonomic nervous system, stimulating them to exert indirect cardiac activity such as diminished impulse conduction rate through the atria and atrio-ventricular node (vagotonic) and senzitisation of the carotid sinus nerves (sympathomimetic). Indirect cardiac contractility changes also result from changes in venous compliance brought about by the altered autonomic activity and by direct venous stimulation. The interplay between direct and indirect activity governs the total circulatory response, which is not identical for all subjects. In the presence of certain supraventricular arrhythmias, the neurogenically mediated slowing of AV conduction is paramount.The degree of neurohormonal activation occurring in patients with heart failure is associated with clinical deterioration and an increased risk of death. Digoxin reduces activation of both the sympathetic nervous system and the (renin-angiotensin) system independently of its inotropic actions and may favourably influence survival. Whether this is achieved via direct sympathoinhibitory effects or by re-sensitizing baroreflex mechanisms remains unclear.
Absorption
Intravenous administration of a loading dose produces an appreciable pharmacological effect within 5 to 30 minutes; this reaches a maximum in 1 to 5 hours.
The major route of elimination is renal excretion of the unchanged drug.
Digoxin is a substrate for P-glycoprotein. As an efflux protein on the apical membrane of enterocytes, P-glycoprotein may limit the absorption of digoxin. P-glycoprotein in renal proximal tubules appears to be an important factor in the renal elimination of digoxin.
INDICATIONS :
DIXISOL is indicated in the management of chronic cardiac failure. The therapeutic benefit of digoxin is greater in patients with ventricular dilatation. DIXISOL is specifically indicated where cardiac failure is accompanied by atrial fibrillation.
DIXISOL is indicated in the management of certain supraventricular arrhythmias, particularly atrial fibrillation and flutter, where its major beneficial effect is to reduce the ventricular rate. DIXISOL is indicated when emergency parenteral digitilisation is required in patients who have not been given cardiac glycosides within the preceding two weeks.
Administration :
Recommended dosages of DIXISOL may require considerable modification because of individual sensitivity of the patient to the drug, the presence of associated conditions, or the use of concurrent medications. Parenteral administration of digoxin should be used only when the need for rapid digitalization is urgent or when the drug cannot be taken orally. Intramuscular injection can lead to severe pain at the injection site, thus intravenous administration is preferred. If the drug must be administered by the intramuscular route, it should be injected deep into the muscle followed by massage. No more than 500 mcg (2 ml) should be injected into a single site. DIXISOL Injection can be administered undiluted or diluted with a 4-fold or greater volume of Sterile Water for Injection, 0.9 % Sodium Chloride Injection, or 5 % Dextrose Injection. The use of less than a 4-fold volume of diluent could lead to precipitation of the digoxin. Immediate use of the diluted product is recommended. If tuberculin syringes are used to measure very small doses, one must be aware of the problem of inadvertent over administration of digoxin. The syringe should not be flushed with the parenteral solution after its contents are expelled into an indwelling vascular catheter. Slow infusion of DIXISOL Injection is preferable to bolus administration. Rapid infusion of digitalis glycosides has been shown to cause systemic and coronary arteriolar constriction, which may be clinically undesirable. Caution is thus advised and DIXISOL Injection should probably be administered over a period of 5 minutes or longer. Mixing of DIXISOL Injection with other drugs in the same container or simultaneous administration in the same intravenous line is not recommended.
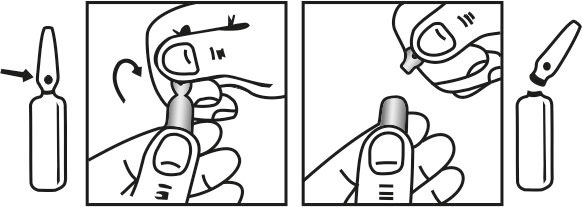
INSTRUCTIONS FOR USE OF AMPOULE :
The ampoule used in this product is equipped with O.P.C (One Point Cut) opening system. No ampoule file is needed to open the ampoule. The neck of the ampoule is prescored at the point of constriction. A coloured dot on the ampoule head helps to orientate the ampoule. Take the ampoule and face the coloured dot. Let the solution at the head of the ampoule to flow down by shaking or a gentle stroke. The ampoule opens easily by placing the thumb on the coloured dot and gently pressing downwards as shown.
Dosage :
In selecting a dose of digoxin, the following factors must be considered :
1. The body weight of the patient. Doses should be calculated based upon lean (i.e., ideal) body weight.
2. The patients renal function, preferably evaluated on the basis of estimated creatinine clearance.
3. The patients age. Infants and children require different doses of digoxin than adults. Also, advanced age may be indicative of diminished renal function even in patients with normal serum creatinine concentration (i.e., below 1.5 mg/dl).
4. Concomitant disease states, concurrent medications, or other factors likely to alter the pharmacokinetic or pharmacodynamic profile of digoxin.
Digitalization may be accomplished by either of two general approaches that vary in dosage and frequency of administration, but reach the same endpoint in terms of total amount of digoxin accumulated in the body.
Rapid digitalization with a loading dose :
DIXISOL Injection is frequently used to achieve rapid digitalization, with conversion to digoxin tablets or digoxin capsules for maintenance therapy. If patients are switched from intravenous to oral digoxin formulations, allowances must be made for differences in bioavailability when calculating maintenance dosages Intramuscular injection of digoxin is extremely painful and offers no advantages unless other routes of administration are contraindicated. Peak digoxin body stores of 8 to 12 mcg/kg should provide therapeutic effect with minimum risk of toxicity in most patients with heart failure and normal sinus rhythm. Because of altered digoxin distribution and elimination, projected peak body stores for patients with renal insufficiency should be conservative (i.e., 6 to 10 mcg/kg). The loading dose should be administered in several portions, with roughly half the total given as the first dose. Additional fractions of this planned total dose may be given at 6- to 8-hour intervals, with careful assessment of clinical response before each additional dose. If the patients clinical response necessitates a change from the calculated loading dose of digoxin, then calculation of the maintenance dose should be based upon the amount actually given. A single initial intravenous dose of 400 to 600 mcg (0.4 to 0.6 mg) of DIXISOL Injection usually produces a detectable effect in 5 to 30 minutes that becomes maximal in 1 to 4 hours. Additional doses of 100 to 300 mcg (0.1 to 0.3 mg) may be given cautiously at 6- to 8-hour intervals until clinical evidence of an adequate effect is noted. The usual
-Table.jpg)
a Daily maintenance doses have been rounded to the nearest 25-mcg increment.
b Ccr is creatinine clearance, corrected to 70-kg body weight or 1.73 m2 body surface area. For adults, if only serum creatinine concentrations (Scr) are available, a Ccr (corrected to 70 kg body weight) may be estimated in men as (140 - Age)/Scr. For women, this result should be multiplied by 0.85. Note : This equation cannot be used for estimating creatinine clearance in infants or children.
c If no loading dose administered.
d 75 mcg = 0.075 mg.
Atrial Fibrillation
DIXISOL is contra-indicated in intermittent complete heart block or second degree atrioventricular block, especially if there is a history of Stokes-Adams attacks. DIXISOL is contra-indicated in arrhythmias caused by cardiac glycoside intoxication. DIXISOL is contra-indicated in supraventricular arrhythmias associated with an accessory atrioventricular pathway, as in the Wolff-Parkinson-White syndrome, unless the electrophysiological characteristics of the accessory pathway and any possible deleterious effect of digoxin on these characteristics have been evaluated. If an accessory pathway is known or suspected to be present and there is no history of previous supraventricular arrhythmias, DIXISOL is similarly contra-indicated. DIXISOL is contra-indicated in ventricular tachycardia or ventricular fibrillation. DIXISOL is contra-indicated in hypertrophic obstructive cardiomyopathy, unless there is concomitant atrial fibrillation and heart failure but even then caution should be exercised if DIXISOL is to be used. DIXISOL is contra-indicated in patients known to be hypersensitive to digoxin or other digitalis glycosides or to any component of the preparation.
Arrhythmias may be precipitated by digoxin toxicity, some of which can resemble arrhythmias for which the drug could be advised. For example, atrial tachycardia with varying atrioventricular block requires particular care as clinically the rhythm resembles atrial fibrillation. Many beneficial effects of digoxin on arrhythmias result from a degree of atrioventricular conduction blockade. However, when incomplete atrioventricular block already exists, the effects of a rapid progression in the block should be anticipated. In complete heart block the idioventricular escape rhythm may be suppressed. In some cases of sinoatrial disorder (i.e. Sick Sinus Syndrome) digoxin may cause or exacerbate sinus bradycardia or cause sinoatrial block. The administration of digoxin in the period immediately following myocardial infarction is not contra-indicated. However, the use of inotropic drugs in some patients in this setting may result in undesirable increases in myocardial oxygen demand and ischemia, and some retrospective follow-up studies have suggested digoxin to be associated with an increased risk of death. The possibility of arrhythmias arising in patients who may be hypokalaemic after myocardial infarction and are likely to be haemodynamically unstable must be borne in mind. The limitations imposed thereafter on direct current cardioversion must also be remembered. Treatment with digoxin should generally be avoided in patients with heart failure associated with cardiac amyloidosis. However, if alternative treatments are not appropriate, digoxin can be used to control the ventricular rate in patients with cardiac amyloidosis and atrial fibrillation.
Patients receiving DIXISOL should have their serum electrolytes and renal function (serum creatinine concentration) assessed periodically; the frequency of assessments will depend on the clinical setting. Determination of the serum digoxin concentration may be very helpful in making a decision to treat with further digoxin, but other glycosides and endogenous digoxin-like substances may cross-react in the assay giving false-positive results. Observations while temporarily withholding digoxin might be more appropriate. Patients with severe respiratory disease may have an increased myocardial sensitivity to digitalis glycosides. Hypokalaemia sensitises the myocardium to the actions of cardiac glycosides.
Direct current cardioversion :
The risk of provoking dangerous arrhythmias with direct current cardioversion is greatly increased in the presence of digitalis toxicity and is in proportion to the cardioversion energy used. For elective direct current cardioversion of a patient who is taking digoxin, the drug should be withheld for 24 hours before cardioversion is performed. In emergencies, such as cardiac arrest, when attempting cardioversion the lowest effective energy should be applied. Direct current cardioversion is inappropriate in the treatment of arrhythmias thought to be caused by cardiac glycosides. Rapid intravenous injection can cause vaso-constriction producing hypertension and/or reduced coronary flow. A slow injection rate is therefore important in hypertensive heart failure and acute myocardial infarction.
Laboratory Tests :
Patients receiving digoxin should have their serum electrolytes and renal function (BUN and/or serum creatinine) assessed periodically; the frequency of assessments will depend on the clinical setting.
Pregnancy : Category C
Teratogenic Effects :
Animal reproduction studies have not been conducted with digoxin. It is also not known whether digoxin can cause foetal harm when administered to a pregnant woman or can affect reproductive capacity. Digoxin should be given to a pregnant woman only if clearly needed.
Nursing mothers :
Studies have shown that digoxin concentrations in the mothers serum and milk are similar. However, the estimated exposure of a nursing infant to digoxin via breastfeeding will be far below the usual infant maintenance dose. Therefore, this amount should have no pharmacologic effect upon the infant. Nevertheless, caution should be exercised when digoxin is administered to a nursing woman.
Very rare : Thrombocytopaenia
Very rare : Anorexia
Common : Visual disturbances (blurred or yellow vision)
Very rare : Gynaecomastia can occur with long term administration.
Very rare : Fatigue, malaise, weakness.
Symptoms and signs :
The systems and signs of toxicity are generally similar to those described in the Side effects section but may be more frequent and can be more severe. Signs and symptoms of digoxin toxicity become more frequent with levels above 3.0 nanograms/ml (3.84 nanomol/l) although there is considerable interindividual variation. However, in deciding whether a patients symptoms are due to digoxin, the clinical state, together with serum electrolyte levels and thyroid function are important factors.
Adults :
In adults without heart disease clinical observation suggests that an overdose of digoxin of 10 -15 mg was the dose resulting in death of half of the patients. If more than 25 mg of digoxin was ingested by an adult without heart disease, death or progressive toxicity responsive only to digoxin-binding Fab antibody fragments resulted.
Non-cardiac manifestations :
Children :
TREATMENT OF OVERDOSAGE :
Manifestations of life-threatening toxicity include ventricular tachycardia or ventricular fibrillation, or progressive bradyarrhythmias, or heart block. Digoxin Immune Fab (Ovine) should be used to reverse the toxic effects of ingestion of a massive overdose. The decision to administer Digoxin Immune Fab (Ovine) to a patient who has ingested a massive dose of digoxin but who has not yet manifested life-threatening toxicity should depend on the likelihood that life-threatening toxicity will occur. Digoxin is not effectively removed from the body by dialysis due to its large extravascular volume of distribution. Patients with massive digitalis ingestion should receive large doses of activated charcoal to prevent absorption and bind digoxin in the gut during enteroenteric recirculation. Emesis may be indicated especially if ingestion has occurred within 30 minutes of the patients presentation at the hospital. Emesis should not be induced in patients who are obtunded. If a patient presents more than 2 hours after ingestion or already has toxic manifestations, it may be unsafe to induce vomiting because such maneuvers may induce an acute vagal episode that can worsen digitalis-related arrhythmias. In cases where a large amount of digoxin has been ingested, hyperkalemia may be present due to release of potassium from skeletal muscle. Hyperkalaemia caused by massive digitalis toxicity is best treated with Digoxin Immune Fab (Ovine); initial treatment with glucose and insulin may also be required if hyperkalaemia itself is acutely life-threatening.
PHARMACEUTICAL PRECAUTIONS :
STORAGE :
24 months from the date of manufacture.
PRESENTATION :